What Every Trauma Treatment That Works Is Quietly Doing
You can feel it before you can name it. The jaw that will not unclench, the shoulders up around the ears, the low hum of alarm that runs underneath an ordinary Tuesday. You have tried to talk yourself down from it. You have heard the advice a hundred times, from friends, from books, from the clinician who meant well: breathe, ground, feel it in your body, be patient with the process. And still, when you close your eyes at night, you can picture the thing that happened as if it were happening again, in color, right now.
There is a reason the list of things you can try for trauma is so long. When something works reliably, the list gets short. Medicine does not keep forty treatments for an infection that penicillin resolves. The length of the trauma treatment menu is itself a confession that most of what is on it does not do the one thing that matters.
This article is about the short list. It is about what the treatments that actually work are all quietly doing underneath their different names, and why that one shared mechanism, visual-spatial tasking, is the part worth understanding.
The long menu of things you can try
Walk into the trauma field as a suffering person and you are handed a catalogue. Talk therapy. Cognitive behavioral therapy. Somatic experiencing. Yoga and breathwork. Neurofeedback. Tapping and energy work. Equine therapy. Psychedelics. Parts work. Journaling prompts and gratitude practices. Each has its advocates, its testimonials, its book on the shelf.
Most of these do something. They soothe. They regulate a nervous system for an afternoon. They build, through repetition, a new pathway between a trigger and a calmer response. That is real and it is useful, and it is also not the same as resolution. A pattern interrupt placed between the trigger and the old reaction is a coping skill. The
affective memory underneath it stays exactly where it was, fully charged, waiting for the day the skill is not fast enough.
That distinction is the whole game. Coping manages the charge. Resolution removes it.
The short list of what actually resolves it
Narrow the catalogue to what the evidence supports and the list collapses fast. The International Society for Traumatic Stress Studies, the field's standard-setting body, published its Prevention and Treatment Guidelines in 2019. For adults with PTSD the strong recommendations are a small cluster: cognitive processing therapy, cognitive therapy, prolonged exposure, trauma-focused cognitive behavioral therapy, and eye movement desensitization and reprocessing, or EMDR.
Sitting just outside those guidelines is a newer protocol with striking numbers. The Reconsolidation of Traumatic Memories protocol, developed by Frank Bourke and first used with survivors of the World Trade Center attacks, has reported over 90 percent of participants scoring below diagnostic threshold for PTSD across independent trials. In a randomized controlled trial of military women, Richard Gray and colleagues found the protocol eliminated intrusive symptoms in the treated group versus none in the controls.
Set EMDR and RTM beside cognitive processing therapy and something strange stands out. They look nothing alike. One has you follow a moving hand with your eyes. One has you run a memory backward in your imagination like a film in reverse. One has you write and reread an account of the worst day. Different rooms, different scripts, different theories of why they help. And yet they arrive at the same place. So the honest question is not which one is best. It is what they share.
The mechanism hiding in the ones that work
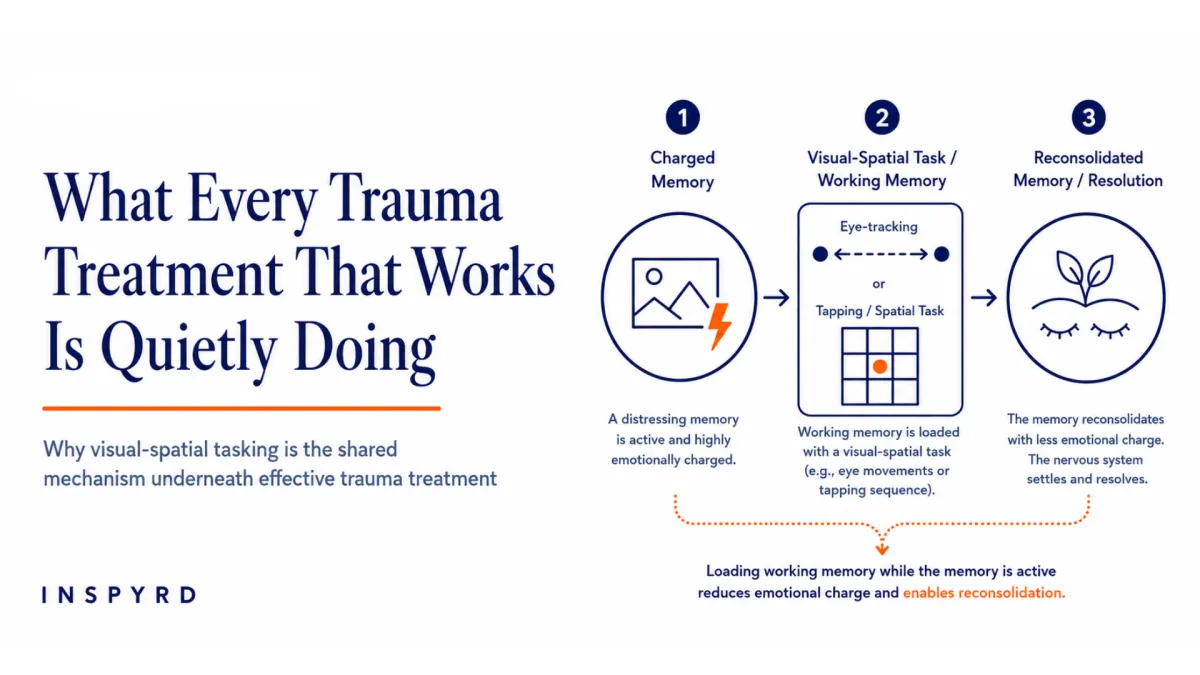
Here is the thread. Every high-efficacy trauma modality, from where I stand, asks the client to hold the charged memory in mind while the working memory is deliberately loaded with a second, demanding visual-spatial task.
This is not a hunch. It has a paper. In 1997, Jackie Andrade, David Kavanagh and Alan Baddeley, working from Baddeley's model of working memory, tested why the eye movements in EMDR seem to help. Their finding, in their own words, was that "images were less vivid with concurrent eye-movements and with a concurrent spatial tapping task that did not involve eye-movements." The eyes were never the point. The point was that a recalled image and a competing visual-spatial task cannot both occupy the limited workspace of working memory at full strength. Load the workspace and the memory goes dim.
Marcel van den Hout and Iris Engelhard spent the following fifteen years testing that claim to destruction. Their conclusion in 2012 was blunt: bilateral stimulation is not
necessary, eye movements as such are not necessary, what is necessary is that the dual task "taxes working memory." Tapping works. Mental arithmetic works. Any sufficiently demanding task works, because the active ingredient was never the specific movement. It was the competition for a scarce resource.
Follow the thread back through the short list and it holds. EMDR taxes working memory with eye movements. RTM taxes it with rapid, structured visual manipulation of the memory, running it backward, changing its size and color and distance. Exposure and cognitive therapies tax it more diffusely, holding the memory in mind while the person does effortful cognitive work on it. The names differ. The engine underneath is the same. This is visual-spatial tasking, whether or not the protocol calls it that.
Why a taxed memory can finally change
Loading working memory does more than dim an image for a session. It opens a window. When an emotional memory is deliberately reactivated, it becomes briefly unstable, editable, before it re-stores itself. Karim Nader and Joseph LeDoux demonstrated this at the cellular level in 2000, showing that "fear memories require protein synthesis in the amygdala for reconsolidation after retrieval." Retrieve the memory and, for a short window, it must be written back to disk. Whatever is true in the workspace during that window is what gets saved.
That is the leverage. Visual-spatial tasking holds the memory open and drains its charge at the same time, so the version that reconsolidates is the calm one. The change is physical, not narrative. Donald Hebb described the underlying rule in 1949: when one cell repeatedly takes part in firing another, "some growth process or metabolic change takes place" that strengthens the connection. Trauma is that rule running in the wrong direction, a threat circuit wired hard. Reconsolidation with visual-spatial tasking is the same rule used deliberately, to rewire it.
And this is why the felt sense matters more than the story. Affective memory is not a story you can tell. It is the felt sense encoded at the time of threat, below language, which is why insight alone never resolves it. You can understand precisely where a fear comes from and feel it just as strongly the next morning. Lisa Feldman Barrett's work on constructed emotion points the same way: the brain builds the present partly from what it has stored, so changing the stored material changes the experience at its root rather than at its surface.
Visual-spatial tasking as the core of Affective Memory Resolution
This is the foundation of the work I train, Affective Memory Resolution. AMR is built on rigorous visual-spatial tasking of short-term working memory, applied at the moment an affective memory is activated and labile. Done well, it drops the subjective distress precipitously. That night the person sleeps, and during REM the sleeping brain does
what it could not do while the memory stayed charged: it separates the emotion from the content and context, and the memory settles into long-term storage as something that can be recalled calmly, in full detail, without the old arousal.
Sleep is not the goal to chase here. Sleep is the marker that the system has stood down. Visual-spatial tasking is the tool that gives the resolution. It is the common factor the effective treatments were already using without always naming it, and naming it is what lets a practitioner do it on purpose, precisely, instead of by accident.
FAQ
Why do so many trauma treatments not work long term?
Most modalities regulate the nervous system or build a new pathway between trigger and response, which is coping, not resolution. They leave the affective memory intact and fully charged. Without visual-spatial tasking during a reconsolidation window, the encoded charge is never actually updated, so the symptoms return when the coping skill is overwhelmed.
What do EMDR, RTM, and exposure therapy have in common?
They look completely different, but each one holds the charged memory in active recall while loading working memory with a demanding visual-spatial task. That competition dims the memory and opens a reconsolidation window. Visual-spatial tasking is the shared mechanism underneath the different names.
Can understanding where my trauma came from resolve it?
Usually not on its own. Affective memory is a felt sense encoded below language, so insight operates at the wrong layer. Resolution comes from updating the memory itself during a reconsolidation window using visual-spatial tasking, which is a physical change in the encoding, not a change in the story you tell about it.
What this means for practitioners
If you already work with trauma, the practical shift is to stop treating your modality as a brand and start treating it as a delivery system for one mechanism. Whatever protocol you were trained in, ask where in it the client's working memory is being taxed while the memory is live, and how cleanly. Sharpen that step and you sharpen your outcomes. Blur it, or skip the reconsolidation window, and you are doing sophisticated regulation while the affective memory sits untouched. The mechanism is the intervention. The name on the door is just the room you happen to be standing in.
Where to take this next
If you are a practitioner who wants to work at the mechanism instead of the brand, the INSPYRD training in NLP and Affective Memory Resolution is where that skill is built. If you are carrying an unresolved memory yourself, know that resolution is possible in a brief series of sessions, and that the tiredness and the alarm are symptoms of something that can be updated, not who you are. Come find the work at INSPYRD.
About the Author
Allen Kanerva is a trauma intervention trainer and the founder of INSPYRD. A former Royal Canadian Air Force tactical helicopter pilot, UN peacekeeping course director, and co-author of Canadian humanitarian security policy work, he developed Affective Memory Resolution (AMR) and Visual-Spatial Tasking (VST), a clinical protocol for nervous-system-level trauma resolution grounded in Hebbian learning and memory reconsolidation research. He trains practitioners internationally in NLP, trauma intervention, and mechanism-first change work.
ORCID ID: 0009-0009-1297-3778
References
Andrade, J., Kavanagh, D., & Baddeley, A. (1997). Eye-movements and visual imagery: A working memory approach to the treatment of post-traumatic stress disorder. British Journal of Clinical Psychology, 36(2), 209-223.
This is the origin study for the working-memory account of EMDR. Andrade and colleagues showed that both eye movements and a non-ocular spatial tapping task reduced the vividness and emotionality of distressing images, isolating the visuospatial sketchpad of working memory as the site of action. It is the paper that establishes visual-spatial tasking, not eye movements specifically, as the mechanism, which is the central claim of this article.
van den Hout, M. A., & Engelhard, I. M. (2012). How does EMDR work? Journal of Experimental Psychopathology, 3(5), 724-738.
This review and experimental program tested competing explanations for EMDR and concluded that the essential requirement is a dual task that taxes working memory, not bilateral stimulation or eye movements as such. It supports the article's core argument that different high-efficacy modalities converge on one mechanism. It also justifies treating visual-spatial tasking, rather than any single protocol, as the active ingredient worth training deliberately.
International Society for Traumatic Stress Studies. (2019). Posttraumatic stress disorder prevention and treatment guidelines: Methodology and recommendations. ISTSS.
The ISTSS guidelines are the field's standard-setting evidence synthesis, and they anchor the article's claim that the list of what actually works is short. Their strong recommendations for cognitive processing therapy, cognitive therapy, prolonged exposure, trauma-focused CBT and EMDR define the "short list"
examined here. Placing these named treatments side by side is what makes the shared mechanism visible.
Gray, R., Budden-Potts, D., & Bourke, F. F. (2019). Reconsolidation of traumatic memories for PTSD: A randomized controlled trial of 74 male veterans. Psychotherapy Research, 29(5), 621-639.
This randomized controlled trial supplies the efficacy evidence for the Reconsolidation of Traumatic Memories protocol cited in the article, with a large majority of treated participants losing their PTSD diagnosis. RTM's rapid visual manipulation of the memory is a clear example of visual-spatial tasking under a different name. It supports the article's convergence argument and its claim that resolution-grade outcomes are achievable in brief treatment.
Nader, K., Schafe, G. E., & LeDoux, J. E. (2000). Fear memories require protein synthesis in the amygdala for reconsolidation after retrieval. Nature, 406(6797), 722-726.
This is the foundational demonstration that a retrieved memory becomes labile and must be actively reconsolidated to persist. It provides the biological basis for the article's claim that a reactivated memory opens a window in which change is possible. Without reconsolidation, visual-spatial tasking would only dim a memory temporarily rather than update it durably.
Hebb, D. O. (1949). The organization of behavior: A neuropsychological theory. Wiley.
Hebb's rule explains why trauma wires a threat circuit hard and why deliberate reconsolidation can rewire it. His description of a "growth process or metabolic change" strengthening connections between co-firing cells is the learning principle underneath both the injury and its resolution. The article uses it to frame trauma as a physical encoding that can be physically updated.
Barrett, L. F. (2017). How emotions are made: The secret life of the brain. Houghton Mifflin Harcourt.
Barrett's theory of constructed emotion supports the article's claim that the brain builds present experience partly from stored material, so updating the stored affective memory changes the felt experience at its root. It reinforces why insight at the level of story is insufficient. Her framework informs the Future Pacing and encoding-layer reasoning within Affective Memory Resolution
